BIO 442 MENU
syllabus 
1 - genome
2 - mutate
3 -cell cycle
4 - karyotype
5 - chromoabn
6 -sex-determ
7 -prenatal
8 - mendelian
9 - complex
10 - non-trad
11 - clinical
12 - newborn
13 - teratog
14 - linkage
15 - DNA prof
16 - quanti
17 - links
18 - quizzes
(full title of lecture appears in status bar on the top or at the bottom of your window)

Biology 442 - Human Genetics
Prenatal Diagnosis and Genetic Counseling
Prenatal Diagnosis. Autosomal aneuploidies are correlated with maternal age. Pregnant women who are 35 years or older are counseled for advanced maternal age (AMA) and offered ultrasound to determine gestational age and amniocentesis between 15-20 weeks. The risk of a miscarriage from amniocentesis is about 1/200 and the risk of the procedure is less than the risk of a fetus with a chromosome abnormality is greater beginning at 34 to 35 years of age. Therefore, amniocentesis, a procedure which removes about 15-20 ml of amniotic fluid from around the fetus, is routinely offered for AMA. The fluid contains amniotic fluid cells which are then cultured and karyotyped. AFP level in the amniotic fluid is also determined to detect any abdominal wall defects (AWD) or neural tube defects (NTD). The amniocytes can also be used in DNA analysis for fetuses at risk of a genetic disorder. The detection rate for chromosome abnormalities by amniocentesis is virtually 100%. Early amnios can be done at 12-14 weeks with a risk of 1/100 or a chorionic villus sampling (CVS) can be done at 10-12 weeks with a risk of 1-3/100.
The California Expanded Maternal Serum Alpha Fetoprotein Screening (MS-AFP) was implemented to detect chromosome aneuploidies in both younger and older women who decline amniocentesis. The detection rate for Down syndrome by MS-AFP is 66% and for trisomy 18, the detection rate is 60%. This program takes maternal blood samples of all age women who are in the 15th to 20th week of pregnancy. It is a screen and not a test. It uses measurements of alpha-fetoprotein (AFP), a normal fetal blood protein, human chorionic gonadotropin (hCG), the same hormone measured in pregnancy tests, unconjugated estriol (uE3), and age to come up with a risk for chromosomal abnormalities (trisomy 21, trisomy 18, monosomy X) and for neural tube defects (NTD), anencephaly or abdominal or ventral wall defects (AWD or VWD) such as gastroschisis or omphalocoele. Race, smoking, and weight are also factors in the risk determination. This is a relatively non-invasive test since it only depends on drawing blood between 15 and 20 weeks of gestation. The accuracy is only about 66% for detecting trisomy 21, however, for NTDs and AWDs, it is much more sensitive. The detection rate for open spina bifida is 80%, for anencephaly, 97% and for abdominal wall defects, 85%. The screen is also called the triple marker screen.
COMMON MS-AFP PATTERNS
|
AFP
|
hCG | uE3 |
Condition
|
| lo | hi | lo | Down syndrome, dates less advanced, Turner syndrome with cystic hygroma |
| lo | lo | lo | trisomy 18 |
| hi | nl | nl | open spina bifida, abdominal wall defects, fetal death |
| hi | nl | lo | anencephaly |
| hi | lo | hi | dates more advanced |
| nl | nl | very low | fetal death, X-linked ichthyosis (placental sulfatase deficiency), congenital adrenal hyperplasia, Smith Lemli Opitz Syndrome |
Amniocentesis, early amniocentesis and chorionic villus sampling are more invasive but more accurate procedures for chromosome abnormalities and gene mutations which can be detected by enzyme assay or DNA analysis.
The combination of two new noninvasive methods to screen for Down syndrome promises 94% accuracy and thus approaches the accuracy of CVS and amniocentesis, both more risky procedures. A recent study has been done which is called the First and Second Trimester Evaluation of Risk (FASTER). It calculated the accuracy of using a combination of maternal blood tests and ultrasound to detect Down syndrome. The first trimester blood screen uses measurements of PAPP A (pregnancy-associated plasma protein A) and free beta hCG, the measurement of the thickness of the back of the fetus' neck (a nuchal translucency ultrasound), and includes the mother's age. These measurements are done at 10-14 weeks and the accuracy is 76%. The quad test is a measurement of four fetal proteins or maternal hormones: hCG, estriol, alpha-fetoprotein and inhibin-A between 15-18 weeks; its accuracy is 84%. The integrated test (FASTER) includes the combined and the quad tests and the resulting accuracy is 94%.
Ultrasound
These procedures are all preceded by a high resolution ultrasound to determine gestational age by size, the number of fetuses, to examine the internal organs such as the heart, kidneys, stomach, intestines, bladder, look at external structures such as appendages, face, head, digits, and the placenta and its location. Ultrasound is also used to guide the physician who will do the CVS, early or regular amnio. Ultrasound between 15 to 20 weeks can pick up 95% or more of the NTDs and anencephaly. Ultrasound can detect both polyhydramnios (too much amniotic fluid) or oligohydramnios (too little fluid) both of which often indicate a problem in the fetus.
Amniocentesis
Regular amniocentesis is done between 15 and 20 weeks of gestation and carries a risk of 1 in 200 of a miscarriage as a consequence of the test. The Rh blood type of all women undergoing either amniocentesis or CVS (see below) must be known. Rh negative women receive Rhogam (Rh immune globulin) after these invasive procedures to prevent Rh sensitization (immunization) in the mother. About 15 ml of amniotic fluid is removed which the fetus replaces in a few hours. The fluid is the color of urine (which it resembles in composition) and it contain fetal cells sloughed off the skin or urinary bladder. Early amnios are done before 15 weeks between 12 and 14 weeks usually but only when there is enough fluid to remove. The risk of miscarriage is somewhat higher, about 1%. Both regular and early amnios are usually done trans abdominally but can be done trans cervically.
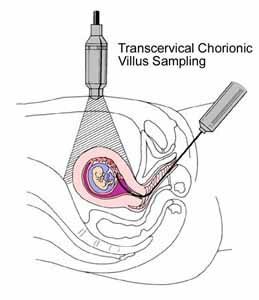
Chorionic Villus Sampling (CVS)
Chorionic villus sampling (CVS) is done between 10 and 12 weeks with a higher risk than for amniocentesis (1/100 risk of miscarriage). When done too early, it has been associated with limb defects in the fetus, probably due problems caused by vascular disruptions and subsequent problems in the fetal circulation. The procedure is usually done though the vagina and cervix but can be done transabdominally. A piece of the chorionic villi is removed and the maternal cells dissected away. Even so there is always a chance of maternal cell contamination, however, cytogeneticists have methods for detecting it. A direct cell preparation can give preliminary results since there are many dividing cells in this tissue. However, the CVS cells are also cultured and examined as is done for amniotic fluid cells. CVS tissue is extra embryonic and the selection against chromosome abnormalities is not so great, therefore, one often sees confined placental mosaicism (CPM). CPM describes the situation in which there is a normal cell line and a cell line with a chromosome abnormality in the CVS cultured cells. When this happens, an amnio is recommended between 15 and 20 weeks gestation. There was a case of trisomy 15 in a CVS sample and a normal diploid cell line on amniocentesis where later it was discovered that the two chromosomes 15 came from the mother, uniparental disomy, UPD. In this case, the child had Prader Willi syndrome which is caused by the lack of a paternal allele on chromosome 15 which is needed for normal development.
Pseudo Mosaicism and Confined Placental Mosaicism
Pseudo mosaicism is the term used for abnormal cell lines that occur after cell culture and which are seen only in the progeny of one colony of cells (usually several cell cultures are prepared from any one amniotic or CVS sample).
Confined placental mosaicism is a term used to describe the situation when a chromosome abnormality may be present in a placenta but not in the fetus). In the first week after conception, only a few cells will give rise to the embryo proper, therefore, a post zygotic (mitotic) non disjunction may involve only the extra embryonic membranes (chorion or amnion) or only the fetus. In the first case, the placenta may come to be totally aneuploid or mosaic for the aneuploidy, while the fetus is normal (confined placental mosaicism). However, a completely trisomic placenta may be structurally and functionally abnormal, possibly leading to loss of a normal (euploid) fetus. The second case would result in the reverse situation with a normal or mostly normal mosaic cell line in the placenta with a fetus that is aneuploid. This situation where the extra embryonic membranes are diploid (or mostly diploid) and the fetus is trisomic or monosomic in the case of XO might promote the survival of some aneuploidies that would normally die.
A situation can arise where the placenta is trisomic and the fetus is diploid but has heterodisomy or isodisomy. As mentioned earlier, UPD, can arise from either trisomy or monosomy rescue. There has been a case of trisomy 16 rescue. DNA analysis showed the mother was heterozygous for two "markers" (RFLPs) on chromosome 16 and the father was homozygous for a different marker at the same site. The CVS was trisomic and DNA analysis showed all three markers (both of the mother's and also the father's). A subsequent amniocentesis which analyzed the amniotic fluid cells from the fetus was diploid and DNA analysis showed the two markers found in the mother and the CVS but none from the father. Therefore, the "normal" diploid fetus was actually heterodisomic for chromosome 16. Since there were both of the mother's markers, the non disjunction occurred in maternal meiosis I. (If only one of the mother's markers had shown up but in a double dose, and none of the father's, then it would have been isodisomy and due to a maternal meiosis II error.)
Ultrasound (US) can detect most NTDs and AWDs but not all. Amniocentesis is the only test for chromosome abnormalities that is 100% correct (except for rare cases of maternal cell contamination or mixed up cultures). Amniocentesis can also detect AFP leaked directly from the baby and AChE (Acetyl choline esterase) a CNS specific enzyme to pick up NTDs that are too small to see on US. This is especially important for women who screen positive for NTD but for whom it US does not detect an AWD or NTD.
Unexplained high (>2.50 MoM) AFP and hCG (> 2.0 MoM) results are known to be an indication of certain pregnancy complications such as prematurity, preeclampsia, and fetal demise.
In practice, the most common reason for a positive screen result is incorrect estimation of gestational age at the time the blood is drawn. Therefore, an ultrasound is done when the woman with a positive screen is counseled in the state approved and certified Prenatal Diagnostic Center. Only board certified ultrasonographers, amniocentesis practitioners and genetic counselors are allowed by the state to participate in the MS-AFP program.
