BIO 442 MENU
syllabus 
1 - genome
2 - mutate
3 -cell cycle
4 - karyotype
5 - chromoabn
6 -sex-determ
7 -prenatal
8 - mendelian
9 - complex
10 - non-trad
11 - clinical
12 - newborn
13 - teratog
14 - linkage
15 - DNA prof
16 - quanti
17 - links
18 - quizzes
(full title of lecture appears in status bar on the top or at the bottom of your window)

Biology 442 - Human Genetics
Teratogens
The word, teratogen, is derived from "terato" meaning monster and "gen, " to give rise to, so teratogens give rise to monsters (not really). Teratogens are non-genetic factors that interfere with normal embryonic and fetal differentiation and morphogenesis. They are not mutagens. Mutagens act randomly on all DNA and do not produce one specific genotype. Children who have been exposed to teratogens in utero will not pass their defect on to their children. Because the effects of teratogens are seen at birth and are therefore a congenital defect, they are often thought to be genetic and can mimic genetic disorders. But we know that congenital does not mean genetic and genetic does not mean congenital.
The study of teratogens is part of training in human genetics because it is important to distinguish the problems they cause from genetic disorders. They are also important because they can be prevented by education of the community. Fetal death, prematurity, growth retardation, and unexplained dysmorphology are all suggestive of teratogenic effects.
The four important factors in teratogenicity are
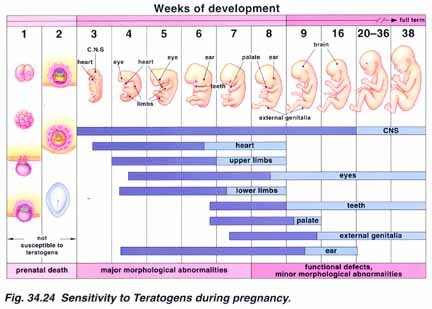
1. Time, the gestational age of the fetus at the time of the exposure to the teratogen. Different organs of the body are forming at different times and therefore the sensitivity to the teratogen and the affected organ will vary. There is an "all or none" period in the first two weeks where the fetus is generally not susceptible to teratogens.
2. Dosage. To how much of the teratogen was the fetus exposed.
3. The genotype of the fetus. The fetus may be more or less resistant to the teratogen because of inactivation of the teratogen.
4. The genotype of the mother. Mothers also differ in their ability to detoxify the teratogen.
Common teratogenic agents and their syndromes include alcohol (most common) and fetal alcohol syndrome (FAS); cocaine and CNS defects; smoking and miscarriage, low birth weight, MR, prematurity and SIDs; uncontrolled diabetes and caudal regression, cardiac and NTD defects; Isotretinoin (retinine for acne) and fetal loss, head, ear, CNS abnormalities, rubella and deafness, varicella and limb defects, skin scarring, PKU and MR, seizure medications and the fetal hydantoin syndrome (FHS); thalidomide and limb defects. There are teratogen registries and all street drugs and medications have been classified into categories A,B,C,D,X where A and B show no evidence of risk and C, D, and X show evidence of risk in increasing certainty. The information often comes from retrospective and uncontrolled studies so information is usually not complete although a few are well documented.
Teratogen List
Anticonvulsants
Fetal Hydantoin Syndrome. No anticonvulsants are completely safe; 5 have similar phenotypic pattern. 7-15% risk of recognizable effects; risk of subtler effects may be higher
"Anticonvulsant facies" narrow bifrontal diameter; short nose; hyperplasia; long philtrum; hypertelorism; up slanted eyes; cupped helix of ear; inverted V of eyebrow. Nail hypoplasia; proximal thumbs. Prenatal growth deficiency; microcephaly
12 - 15 % of women on anticonvulsants will have babies with none of these
Dilantin (Phenytoin) risk for Fetal Hydantoin Syndrome is 10% and for having some effects is 33%. 2 to 3 X greater risk for child with congenital defects over general population. Typical craniofacial defects and variable degrees of hypoplasia and ossification of the distal phalanges. Impaired growth, both physical and mental, congenital heart defects and CL and/or CP are often seen in conjunction with FHS. 38% had IQ 79. It is considered the safest for use in pregnancy. However, because there appears to an increased risk of malformations and birth defects in women taking phenytoin it should be used in pregnancy only if the physician feels that the potential benefit outweighs the risk.
Trimethadone syndrome is similar to Dilantin
Fetal valproate effect is similar to Dilantin (had been thought to be safe) (Depakote or Depakene) Refer immediately to MSAFP Program if taken during the 1st trimester or 1 month prior to conception. Prenatal growth deficiency; MR; typical facies; nail hypoplasia; cardiac defects;, NTD risk is 1-2% = 10 X general population. Delivery--distressed labor 50%; Low Apgar scores 28%
Carbamazepine (Tegratol) is similar to Dilantin. People on this medication are referred immediately to the XMSAFP Program if the medication was taken during the 1st trimester or 1 month prior to conception. Prospective study showed incidence of 3 minor malformations was higher. Major malformations included NTD but probably < than Valproic Acid but still 1% risk; growth deficiency. Developmental delay 23%
Mysoline. Similar facial defects; nail hypoplasia; prenatal growth deficiency; microcephaly.
Phenobarbitol is not safe for pregnancy. Microcephaly but no growth deficiency; developmental delay 20%. 38% had 3 or > minor malformations. No increase in major malformations. Baby may have withdrawal symptoms/bleeding (needs Vit K). Similar cranial facial defects and nail hypoplasia to others
Antipsychotic drugs and tranquilizers
Benzodiazepines. Valium (diazepam) had been reported earlier (1975) that there were > CL±CP and > CP. Later studies (1983,84,88) say they do not cause increase in oral clefting in 1st trimester although cannot say they are not teratogenic because they have not been studied nor has librium. Jones is studying Prozac.
Phenothiazines (thorazine) for psychosis. 1977 was last study . Risks low if used occasionally in small doses. Some of them seem to be teratogenic; sporadic reports of birth defects. Use near term may be associated with maternal hypotension and infant hypotonia.
TRICYCLIC ANTIDEPRESSANTS (imipramine) appear not to be teratogenic
Lithium. Estimates cited in older literature appear to be too high: 11% malformed; 8% major cardiovascular defect; 2.7% tricuspid valve (Ebsteins Anomaly) which is very rare in general population 1/20,000). Their studies at UCSD showed an increase in > Ebstein's Anomaly but not as high as previous study indicated. Best estimates for congenital heart disease in these babies are in the 1-5% range .Greatest risk is in 1st trimester.
Antimicrobials
antibacterials
Apparently not a problem with prenatal exposure. Except aminoglycosides have ototoxicity both pre and postnatally. TETRACYCLINE after 4th month causes abnormalities of deciduous teeth (not permanent teeth)
Antituberculous. Isoniazid needs to be supplemented with Vitamin B
antiviral. Acyclovir has possible problems; recommend not to use
Amantadine and ribavirin okay
antifungal--no documented problems
antiparasitic. Chloroquine possible ototoxicity. Primaquine can cause hemolysis in G6PD deficiency. RID Pyrethrins with Piperonyl Butoxide is better than Kwell (Lindane) since it is not absorbed. Kwell is absorbed. Flagyl may be of concern but no proof it that causes problems
Antihypertensives
Sympatholytics: Have not been studied for 1st trimester; only during 3rd trimester when blood pressure is higher. Methyl-dopa a2-adrenergic agonist has been studied very well and is okay. Propanolol, adrenergic antagonist carefully studied and is okay to use
Vasodilators: Hydralazine has been studied and is okay
Minoxidil (which is used for baldness) causes hairy babies (hypertrichosis)
Sodium Nitroprusside probably should not be used
Angiotension converting enzyme inhibitors (ace inhibitors). Captopril and Enalopril lead to renal dysplasia and Potters Syndrome--infants born with severe renal and pulmonary hypoplasia; greater problem when given in 2nd and 3rd trimester when the kidney forms
Anticoagulants
Warfarin (coumadin). Prenatal growth deficiency; developmental delay. Seizures (2nd or 3rd trimester). Hypoplastic nose; stippled epiphyses. 2/3 of fetuses of women on coumadin have 1 or > of these defects. The 6th and 7th week is critical period for some of these malformations. Conflicting evidence for 2nd and 3rd trimester. Can use heparin instead. Skeletal defects probably due to the inhibition of ARSE (arylsulfatase E) which is deficient (mutation) in chondrodysplasia punctata (mendelian trait) both are characterized by aberrant bone minerlization, severe underdevelopment of nasa cartilage and distal phalangeal hypoplasia. (Phenocopy)
Heparin complications of pregnancy are due to the disease not heparin. It does not cross placenta, not associated with birth defects. May have miscarriage or prematurity, stillbirth.
AMINOPTERIN Used as an abortifacient. Folic acid antagonist may cause leukemia.
ACCUTANE AND VITAMIN A. Accutane or isotretinoin. Severe problems--potent human teratogen. SAB 22%; malformed. stillborn 3%; malformed liveborn 11%. Malformations of head and face, CNS, thymus and heart. Cranial facial defects include absence or hypoplasia of external ear (microtia). Congenital heart disease; thymic defects; CNS hydrocephalus and microcephalus; cortical blindness
Tretinoin (all-trans-retinoic acid) is fat soluble and can hang around longer than accutane, can get embryopathy even after being off the medication for a year. Accutane seems to be okay if stopped before conception
Vitamin A. Excess Vitamin A (above RDA of 2,700 IU); Vit A supplements often contain 10,000 IU. 3.2% of infants born to women who had taken 10,000 IU had CL/CP hydrocephalus, or major heart defects compared to 1.3% babies born to women who took 5,000 IU. Other defects seen include CNS, limbs and cardiovascular system as well as behavioral abnormalities. Since Vit A is fat soluble, excessive doses prior to conception may also cause problems. Excess beta carotene (precursor to Vit A) did not cause an increase in birth defect
Alcohol and drug abuse and the fetus
FAS = fetal alcohol syndrome. Chronic alcohol abuse is the largest public health problem. FAS 1-3/1000 live births; may be 1/40 in some populations.Pattern: Performance--pre and post natal growth deficiency; developmental delay; lissencephaly; decreased brain development and growth; 2 primary brain development problems are abnormal migration of neurons and cell death--this leads to microcephaly and hydrocephaly. Craniofacial--microcephaly; CP; short palpebral fissures; micrognathia; small midface; epicanthal folds; short, small nose; indistinct philtrum (no groove); thin upper lip, low nasal bridge, minor ear anomalies. Limbs--joint contractures; missing or abnormal palmar creases; camptodactyly to Trisomy 18 due to severe problems in brain development. They have a mouse model. Alcohol can affect the embryo at all times during pregnancy. Developmental Problems:Infancy-failure to thrive; growth deficiency; tremulous; irritable; unable to modulate environmental input. Childhood-short attention span; developmental delay; speech delay; motor incoordination. Early School Years-repeat kindergarten; poor peer relationships; impulsivity; poor attention; Developmental delay continues. Middle School-truancy; drop-out; impulsivity; lack of social sensitivity; dental problems needing orthodontist; esotropia (eye migration). Intellectual Functions (ongoing follow-up) 58% IQ 70. Socialization 6 years old for 17 year old
FAE = fetal alcohol effects. 11% of children of women who use 1-2 oz of absolute alcohol/day (2 beers or 8 oz wine) during the 1st trimester have FAE. twice the rate of SAB.
Prenatal cocaine exposure and fetal vascular disruption. 85% of fetal exposure to illicit drugs is to cocaine; most use several other drugs also. Problems are probably due to vascular disruption: prematurity; growth deficiency; microcephaly; developmental delay; SABs; intracranial hemorrhage; limb reduction; cardiac anomalies; hemangiomata. Cocaine is similar to local anesthetics in chemical structure; lipophilic so stays in fetus blocks uptake of serotonin, etc. and leads to vasoconstriction and vascular disruption
CNS stimulation. Route of intake irrelevant--only amount is important. Gets into breast milk and can cause convulsions. Use in first trimester may not be a problem if they quit when they find out they are pregnant; but heavy users especially in second and third trimester see the vasoconstriction problems in the limbs, etc. Level II ultrasound and MSAFP at 16 weeks can pick up some of the consequences of the vascular disruptions such as gastroschisis, etc. Recent studies have shown that substance-exposed babies have twice as much norepinephrine (a neurotransmitter--vasoconstrictive) in their blood than normal babies (no differences found for epinephrine and dopamine, two related neurotransmitters). These babies cry uncontrollably; are jittery, are in continuous motion, are small, have low birth weights despite being term babies. Hypertonicity produces abnormal upper-body stiffness causes crib injuries. Breathing problems place these infants at a relatively high risk for SIDS (also babies exposed to opiates--heroin and methadone). Problems persist at least one year.
Breathing spray paint; Toluene; glue sniffing. Similar to FAS: CNS defects; 56% have pre and postnatal growth and developmental delay; cranial-facial anomalies similar to FAS--71% have micrognathia and abnormal ear placement; 67% have short palpebral fissures; ± flat philtrum; 60% have microcephaly. ± Nail hypoplasia; ± simian palmer crease 11% perinatal demise 40% preterm delivery.
AMPHETAMINES. No clear association with major/minor malformations. Some evidence for withdrawal syndrome in fetus.
HEROIN AND METHADONE. Little objective evidence for association with birth defects
MARIJUANA--THC. No consistent pattern; no major problems. IUGR especially with alcohol use. Limited data on long term behavioral problems.
PCP little data on humans.
SMOKING. Overwhelming evidence shows that maternal smoking during pregnancy has harmful effects on the fetus. IUGR is the most consistent effect. On average, babies born to women who smoke during pregnancy are 200 g lighter than those born to comparable non-smokers. Clear dose-response relationship for this effect. Reductions in birth weight have also been noted in association with "passive smoking" but this finding is controversial. No overall decrease in length of gestation, therefore, reduced birth weight is due to retardation of growth. If smoking is stopped during the first half of gestation, birth weights are virtually normal. Older smokers are at an especially high risk for small for gestational age births, and parous smokers are at an especially high risk for low birth weight infants and preterm delivery.Some studies show smoking affects physical growth, mental development and behavior of offspring. Increases in clefting, ectopic pregnancy, SABs, fetal death and neonatal death. Decreased level of chorionic gonadotropin due to smoking is possible mechanism for greater risk for SABs. Implicated in SIDS. No consistent evidence for increase in congenital malformations. Increased risk of cervical cancer in women.
NITRATES > 15 ppm (in underground drinking water) 4X risk for congenital malformations; musculoskeletal and CNS
Maternal (medical) conditions
Diabetes. Serious risks reported 6-9%; good metabolic control is reported to decrease the risk. Caudal regression malformation complex, transposition of great vessels, renal anomalies, risk for NTDs 4 x greater, CL/CP, macrosomia, perinatal mortality Also, women with gestational diabetes have a 3X greater risk than general population of Type II diabetes after another pregnancy. The risk doubles for every 10 lbs gained after a pregnancy with diabetes.
Maternal PKU. MR, intrauterine growth retardation, microcephaly, congenital heart defects, vertebral anomalies, strabismus, increased fetal wastage. Risk of MR has been estimated as high as 95% with maternal blood phenylalanine concentration of 20 mg/dl or higher.
Systemic lupus erythematosus. Increased risk of fetal loss, congenital heart block--magnitude of risk is not known.
Hyperthermia. Associated with CNS, cardiovascular-atrial septal defects and hypoplastic left heart, NTD, and mild limb bud abnormalities in early gestation. Possible changes in thyroid gland structure during late gestation. Limit hot tub use to 15 min at 390 C; or 10 min 40-41.10 C; Recommend use of antipyretics for febrile illness during early pregnancy. Possible correlation with male infertility
Teenage. Increased risk of gastroschisis. Increased risk of delivering a premature baby independent of social and economic problems, including lack of regular prenatal health care. New studies done on married Utah teens age 13 to 17 who had received adequate prenatal care were twice as likely to deliver a premature infant as similar women age 20 to 24. Teenage mothers were also at risk of having a very small baby. NEJM 4/95
INFECTIONS
Chlamydia. Risk for SAB, low birth weight, stillbirth, premature birth and infant death. Baby can be infected during delivery and is at risk for conjunctivitis and pneumonia.
Toxoplasmosis. Risk of SAB, stillbirth or infant death soon after birth. Affects CNS. An infected baby may appear normal at birth but later develop a defect such as blindness, heart disease or MR.
Chicken pox. (Herpes varicella, Herpes zoster). Congenital Varicella Syndrome: limb hypoplasia, cortical atrophy, skin scarring and eye defects. Clinical manifestations of IU infection in babies without birth defects include skin lesions and pneumonia at birth. One infant developed shingles at 7 mos. Risk to fetus estimated at less than 10% for severe teratogenic effects; critical period id 3-4 months of pregnancy. Rubella. IUGR, FTT, ocular defects, cardiovascular defects, microcephaly, learning disabilities or MR, sensorineural deafness, abnormal ossification of long bones, immune and endocrine disturbances, especially diabetes. Abnormalities vary with month of gestational infection; neurologic signs, endocrine malfunctions and deafness may not be apparent in neonatal period; vaccine available
AIDS. 30% risk to fetus if mother is HIV positive; 50% risk if she has a previous child with AIDS; risk to develop AIDS in infancy, growth retardation, microcephaly, prominent flattened nasal bridge, hypertelorism. Data inconclusive as to whether the virus is a cause of birth defects
Herpes simplex (Types I and II). Primary infection before 20 weeks can lead to increased fetal mortality, microcephaly, seizures, MR chorioretinitis. Most fetal infections acquired at or close to birth; manifestations variable in severity; vaccine currently unavailable but antiviral treatment is available
Bacterial vaginosis. 40% greater chance of giving birth to premature, low birth weight infants than uninfected women.
Contraceptive hormones
Diethylstilbestrol. Malformation of vaginal epithelium, cervix, and uterus; testicular abnormality (mostly minor, such as epididymal cysts); fertility not impaired. Increased risk of vaginal adenocarcinoma and testicular malignancy.
Other estrogens. Possible effects on sexual differentiation and later sexual behavior. Often used with progestins and difficult to sort out the effects
Progestins. Masculinization of external genitalia in female fetuses and feminization of male fetuses; increased risk for hypospadias. Risk estimated at 1-2% before 12th week of gestation, uncertain after 12 week. Some suggestion of increased congenital heart disease unconfirmed.
Estrogen/progestin combinations. Possible genital malformations, and implicated as cause of VACTERL association (vertebrae, anus, heart, trachea esophagus, kidney and limb defects)
Radiation exposure
Ionizing radiation is mutagenic; carcinogenic; and teratogenic. rad = absorbed dose. 100 rads between 2 and 4 weeks when organogenesis is occurring is the most significant time. 200 rads either early death or >>malformations. 250 rads causes multiple problems. 5 rads no problem; 5 - 10 rads ?; 10 rads have problems; (this may be moved to 20 rads). 20 rads may be newer allowable level although 10 rads is cutoff figure given in literature for safety to fetus. Must take mother's need into account. Must go to radiation physicist to get true rad exposure to give accurate counseling.
Stages of development and radiation 1. Preimplantation Day 8-9: All or none effect
2. Organogenesis Day 10 to 9 weeks: Malformations
3. Fetal Period Week 9 to term: Brain is susceptible; cellular hypoplasia (fewer cells); smaller brain and MR; greater risk of leukemia.
